
Patient and Professonal Tools
Nephrology is an ever-evolving field, and we want to share some of its highlights. We have compiled some great resources for you! Check them out:
-
My Kidney Life Plan

Use this free tool to see how dialysis, transplant, or comfort care may impact your life. Your treatment is your choice, we can help you choose the right treatment for YOU.
Try our tool »
-
Dialysis Health Tracker

A simple way to track symptoms, blood results, stock levels, and daily treatment notes in one place. Show nurses and doctors real‑time information.
Try the app »
-
Preventing and Managing PD Complications and Emergencies

Help your PD patients learn to identify red flags, avoid turning a dry contamination into a wet contamination, and be able to explain PD and the type of infection they may have to ER staff who may not know PD at all.
View Courses »
-
Managing Home Hemodialysis Emergencies
Preventable emergencies often involve a cascade of errors that can be headed off when patients know what to watch for. Learn how to teach them to prevent the preventable—and prepare for the unpredictable.
View Courses »
-
Preventing Home Hemodialysis Complications
An ounce of prevention is worth a pound of cure. Learn how to prepare—not scare—patients so they recognize and report issues before they turn into complications, and can respond appropriately if complications do occur.
View Courses »
-
Training for Home Dialysis Success (PD & Home HD)

Training successful home dialysis patients needs to include far more than how to use a machine. How can you support them to be competent and confident in their skills? In this course, you will learn how to tap into your patients’ motivation to help them go—and stay—home.
View Courses »
-
Setting Patient Expectations for Home Dialysis (PD & Home HD)
In this course, you will learn practical ways to help patients find their best lifestyle fit treatment(s), assess them for clinical suitability, conduct home inspections, and empower your patients to take responsibility for as much of their own treatments as possible.
View Courses »
-
Integrating Home Dialysis into Life (PD & Home HD)
Reducing the burden of care is essential to help patients dialyze to live—not live to dialyze. In this course, you will learn how to help patients navigate training and the first few stressful months at home, and make their treatment schedules fit their lives.
View Courses »
-
Setting Staff Expectations about Home Dialysis (PD & Home HD)
PD and home HD are very different than in-center HD. Instead of doing tasks for patients, you’ll teach them how to do their own care—using an empowerment approach. In this course, you’ll learn how to make the shift and equip your patients to do PD and home HD safely.
View Courses »
-
Preventing Early PD Dropout
Research identifies PD catheter dysfunction, infection, early membrane failure or ultrafiltration failure, and psychosocial factors as preventable causes of early PD dropout. Learn how to identify, prevent, or address each of these in this course.
View Courses »
-
Preventing Early Home HD Dropout
Home HD training is a costly nursing time investment for clinics. Both patient- and clinic-level factors play key roles in the likelihood of early home HD dropout. Learn what these are and how to prevent them in this course.
View Courses »
-
The “Flip” – Switching from PD to Home HD
In this course, you will learn practical ways to help patients find their best lifestyle fit treatment(s), assess them for clinical suitability, conduct home inspections, and empower your patients to take responsibility for as much of their own treatments as possible.
View Courses »
-
Talk About Home Dialysis
What is the best way to discuss treatment options, and what should you say? This guide will help make that challenging conversation easier.
Download the PDF »
-
MATCH-D
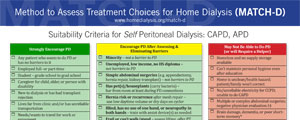
Use our tool to help dialysis staff identify and assess candidates for home dialysis therapies.
Learn more »
-
Core Curriculum for the Dialysis Technician

The Core Curriculum is the industry’s premier, comprehensive training tool to help dialysis technicians—and nurses—learn to provide safe, sensitive, high-quality care for people with end-stage renal disease. Easy-to...
Purchase now »
-
Medicare Start Date Calculator

When does Medicare start for home dialysis vs. in-center? Find out!
Calculate your Medicare start date »
-
Buttonhole: A how-to manual

Patients who self-cannulate have better access outcomes; they take ownership of their care and control of their lives.
Read the article »
-
Ultrafiltration Rate Calculator
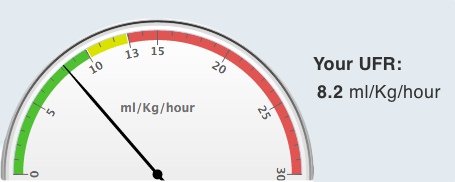
Help your patients SEE how their fluid gains and treatment time affect them. Clinician/expert dialyzor version coming soon!
Calculate your patients UFR »
-
PATH-D PD
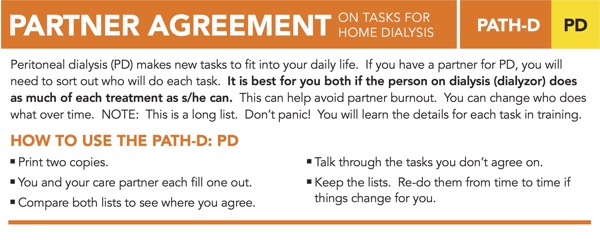
What do your patients and partners expect their roles to be in PD? This new tool can help them communicate.
Download the PDF »
-
PATH-D HHD
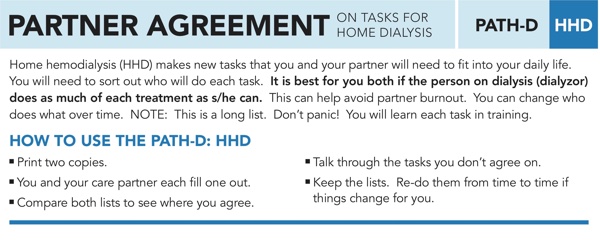
What will your home HD patients do, vs. their partners? Use the PATH-D-HHD to get them on the same page.
Download the PDF »
-
Dialyze to Live

Help YOUR patients to see how full life can be with PD and home HD. Free booklet pdf features active people who are doing well.
Download the PDF »
-
PATH-D PD Español
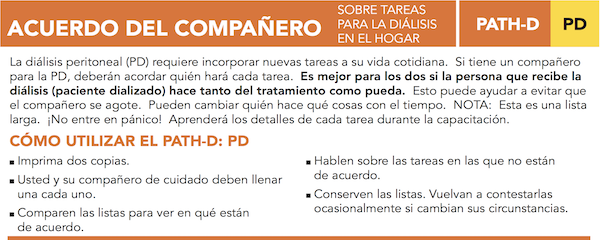
¿Qué esperan sus pacientes y socios de sus roles en la DP? Esta nueva herramienta puede ayudarlos a comunicarse.
Descargar el PDF »
-
PATH-D HHD Español
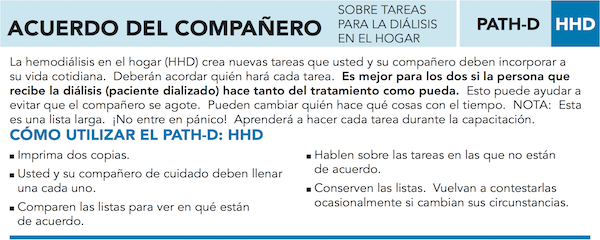
¿Qué harán sus pacientes de HD en casa, frente a sus parejas? Use la PATH-D-HHD para ponerlos en la misma página.
Descargar el PDF »
-
Free postcards

Use our postcards to share Home Dialysis Central with your patients or other renal professionals.
Order now »
-
ETC Selected Clinics
ETC Selected Clinics by State City (Last Updated At: 01-2021).
Download now »
-
CE Courses for Nurses/Technicians

Supporting Home Dialysis Patient's Travel: The Nurses Role
View CE Courses »
Watch on YouTube »
When and How to Bill for Retraining Home Patients
When a Medicare patient needs dialysis, a clinic that is certified to provide home training and support can bill Medicare for a certain number of training sessions. Learn how and when to bill Medicare for retraining.
Message Boards
Talk to other professionals and share your thoughts, concerns, or suggestions about Peritoneal Dialysis or Home Hemodialysis.