How Are You Scoring and Using the KDQOL-36™ to Plan Care?
The Regulatory Mandate & Why It Matters
 The
ESRD Conditions for Coverage under the Condition for Patient plan of
care at 42 CFR 494.90(a), which applies to all dialysis
patients—in-center,
The
ESRD Conditions for Coverage under the Condition for Patient plan of
care at 42 CFR 494.90(a), which applies to all dialysis
patients—in-center,
PD, and home HD states: “(6) Psychosocial status. The interdisciplinary team must provide the necessary monitoring and social work interventions. These include counseling services and referrals for other social services,
to assist the patient in achieving and sustaining an appropriate psychosocial status as measured by a standardized mental and physical assessment tool chosen
by the social worker, at regular intervals, or more frequently on an as-needed basis.”
Well-Being Is a Vital Measure
CMS requires dialysis clinics to monitor patients’ mental and physical well-being (health-related quality of life or HRQOL), as multiple studies have found that low HRQOL survey scores predict a higher risk of hospitalization and death. Fresenius research on almost 14,000 patients used the SF-36. (The KDQOL-36™ has 12 questions from that survey.) The study found that each 1 point higher score on the Physical Component Summary (PCS) score predicted a 2% lower relative risk of hospitalization and death. Similarly, each 1 point higher Mental Component Summary (MCS) score predicted a 1% lower relative risk of hospitalization and a 2% lower relative risk of death.1
KDQOL-36: The Recommended Survey
The Interpretive Guidance was written in 2008. At the time, there was an expectation that CMS would start collecting data on physical and mental functioning like it collects other clinical data. For national consistency, the Interpretive Guidance recommended that dialysis clinics use the KDQOL-36 survey, which was endorsed by the National Quality Forum. The KDQOL-36 was found to be psychometrically sound for use with adult dialysis patients age 18 or older on any type of dialysis. Since some dialysis clinics treat pediatric patients, the IG suggested that clinics use a standardized age-appropriate survey for patients under 18.2

KDQOL-36 Survey Frequency & Use
Dialysis clinics and/or social workers needed to know when to administer the survey. Therefore, the IG stated, “’At regular intervals’ means that the assessment survey is administered by the time of the first reassessment (i.e., within 4 months of initiating treatment), and repeated at least annually. Examples of an “as needed basis” would include repeat use of the of the survey with the patient who has a significant life changing event (e.g., loss of spouse, loss of job, recent move to a nursing home) or a change in health status.”3
The IG further stated, “The social worker must have a system for routine use of the assessment survey, evaluation of the results, and incorporation of the survey results into the development and updating of the psychosocial portion of the plan of care.” CMS believed that doing the initial survey at the same time the social worker is doing the reassessment would allow time to administer the survey, discuss scores with the patient, get patient feedback on contributors to positive or negative well-being, and learn what area(s) the patient is willing to work on with the interdisciplinary team (IDT). Then the social worker could present this information to the interdisciplinary team during the plan of care meeting that is supposed to be based on the full IDT reassessment.
For QAPI, dialysis clinics should monitor the percentage of patients who complete the survey during a specified period and the percent of those who refuse, which all patients have a right to do. The IDT should use the survey to identify and develop a plan to address unmet needs. When a patient refuses to take the survey, those needs remain unmet increasing the patient’s risks for poor outcomes. Talking with patients about the survey’s goals—to address unmet needs and reduce risks—may turn an initial refusal into a completed survey.
A clinic’s QAPI goal for refusals might be 20% or less. To calculate the refusal rate take the Number of Patients Refusing the Survey ÷ Number of Patients Offered the Survey. Some patients are excluded from being surveyed and do not have to be counted in the denominator for the clinic. These include patients who:
Have cognitive impairment, dementia, or psychosis (their results may be unreliable)
Are non-English speakers/readers and no language translation or interpretation is available
Are new to the clinic (<3 months) and may be unstable clinically and psychologically
KDQOL Complete Scoring and Analysis4

In 2009, with no outside funding, the nonprofit MEI launched KDQOL Complete, a comprehensive scoring tool to benefit the community, available online by subscription. Annual subscription pricing is based on the number of patients treated by a single dialysis clinic and has not increased in the 17 years since the site went live:
A small clinic (<10 patients) can subscribe for $100/year
A medium sized clinic (11-49 patients) can subscribe for $250/year
A large clinic (>50 patients) can subscribe for $350/year
Providers with 2 or more clinics can form a group and receive a 20% discount.
The survey can be completed in three ways:
Printed survey - The social worker or any dialysis staff member can give the patient a printed copy of the survey to complete and return while onsite at the clinic.
Survey code - The social worker can email the patient a survey code to complete the survey independently online (in English or Spanish).
Read the survey to a patient chairside - The social worker can read the survey to the patient and record the patient’s responses. In fact, this approach can add to the psychosocial assessment and can increase survey participation by visually impaired or illiterate patients.
NOTE: Allowing a patient to take a survey home reduces the chance it will be returned and raises the risk that someone else will complete it, making the results questionable. A one-year subscription allows unlimited survey administrations per patient. Clinics may choose to survey only annually. However, health setbacks could lead scores to decline over time even when the clinic is doing all it can do to address previously identified problem areas. Developing and implementing an intervention after reviewing scores followed by re-surveying may help a patient see benefits and allow clinic staff to take credit for improvements or alter interventions as needed.
KDQOL Complete is case-mix adjusted for age, sex, and diabetes, using data from the Dialysis Outcomes and Practice Patterns study5—an international prospective study of more than 17,000 patients in the U.S., Europe, and Japan. KDQOL Complete helps interpret the results using a color-coded rating where a score in green is above average, yellow is average, and red is below average. (No real patient names are used in any of these images.)
Four KDQOL Complete Reports6
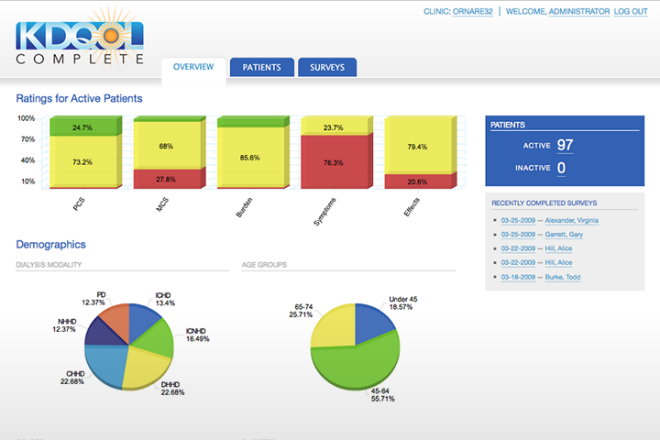 A Clinic Overview report shows
data on the five domains in the survey: physical component
summary, mental component summary, burden of kidney disease,
symptoms/problems, and effects of kidney disease on daily life. This
report can be used for the IDT discussion of clinic level interventions
to address low scores for multiple patients in quality assessment and
performance improvement (QAPI) meetings. For example, a
clinic-level intervention targeted at addressing symptoms/problems could
yield better clinic outcomes for multiple patients and might
improve Quality Incentive Program (QIP) scores and improve revenue by
limiting payment cuts for below average performance.
A Clinic Overview report shows
data on the five domains in the survey: physical component
summary, mental component summary, burden of kidney disease,
symptoms/problems, and effects of kidney disease on daily life. This
report can be used for the IDT discussion of clinic level interventions
to address low scores for multiple patients in quality assessment and
performance improvement (QAPI) meetings. For example, a
clinic-level intervention targeted at addressing symptoms/problems could
yield better clinic outcomes for multiple patients and might
improve Quality Incentive Program (QIP) scores and improve revenue by
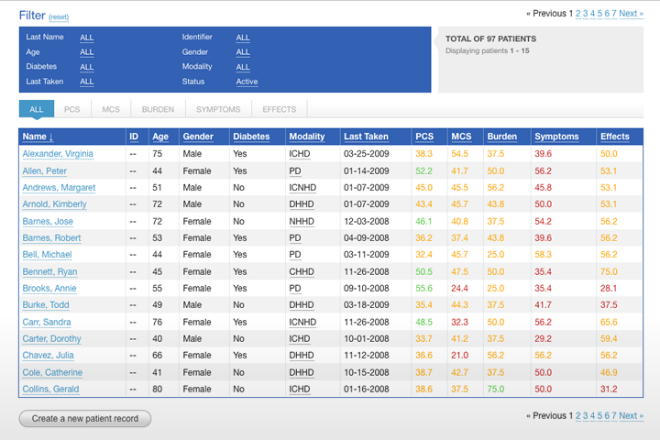
limiting payment cuts for below average performance.A Patient view lists age, sex, diabetes status, treatment type, and scores on the five domains, again color-coded, for all active patients at the clinic. Demographic and treatment data can be edited on this report. A patient can be added, deactivated, and/or moved to another clinic (within your group) in this view. Clicking a patient’s name allows you to view their Patient Summary, which includes editable demographic information and survey history with your clinic. For each survey, there are links to the:
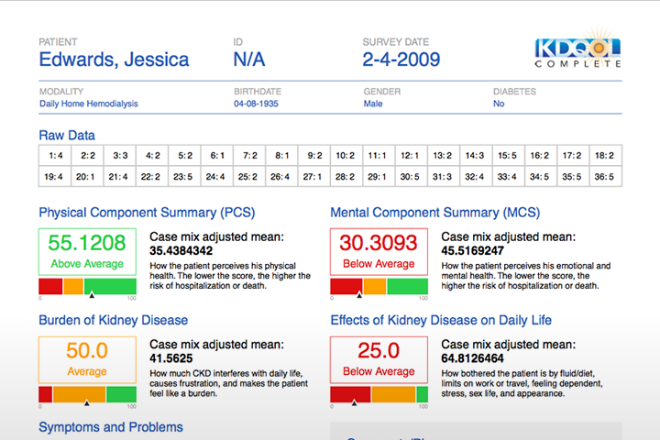 Chart
Report - shows how a patient answered each item,
describes the five domains, and provides a color-coded visual to show
where the patient is doing well and where improvement is needed and IDT
interventions should be considered. Symptoms from the survey are
detailed here, so the IDT knows any that were not communicated to
them.
Chart
Report - shows how a patient answered each item,
describes the five domains, and provides a color-coded visual to show
where the patient is doing well and where improvement is needed and IDT
interventions should be considered. Symptoms from the survey are
detailed here, so the IDT knows any that were not communicated to
them.Patient Report – to be given to the patient. This report will print in any of the languages KDQOL Complete supports. It explains what was measured, their scores, and what they can do to maintain or improve their scores.
Action Plan – developed by a team of dialysis professionals and educators, to suggest steps patients can take to feel better, based on their score and answer combinations.
Education Resources Report - links to free online resources staff and patients can use to address below average scores. One resource is My Kidney Life Plan which could help identify if switching treatment modalities may improve health-related quality of life.
A Score and Rating Trend Report for each patient shows scoring over time by domain.


A Response Trend Report tracks how each patient answers each question over time to help see where targeted interventions might improve scores and reduce risks of hospitalization and death.
Additional KDQOL-Complete Survey Interpretation Resources
An article on the KDQOL Complete home page has background on the survey and tips to administer, score, interpret, and report the results to patients and talk with them about low, average, and above average scores. It also shares some interventions that have been shown to improve scores and tips for incorporating the results into the psychosocial assessment, patient plan of care, and QAPI.
Tools for subscribers include:
A user manual
A Compliance Made Easy article comparing KDQOL Complete to EHR scoring.
The KDQOL-36 in English, Spanish, Chinese (simplified), Tagalog, Korean, French Creole, German, Italian, French, Polish, and Amharic.
Phone or email technical support Monday through Friday.
Conclusion
Social workers who work for clinics that subscribe to KDQOL-Complete or whose clinics previously subscribed until they were acquired by another company have offered high praise for the service and technical support. Some who used both KDQOL Complete and a dialysis company’s scoring program have told MEI that KDQOL Complete saved staff time and provided helpful information they could use with patients and with their team that made their jobs easier. If you haven’t checked out KDQOL Complete, thank you for taking a few minutes to learn about it.
Lowrie EG et al. Medical Outcomes Study Short Form-36: A consistent and powerful predictor of morbidity and mortality in dialysis patients. Am J Kidney Dis 41(6):1286-1292, 2003.↩︎
Centers for Medicare & Medicaid Services. ESRD Surveyor Training Interpretive Guidance Final Version 1.1, October 8, 2008. https://www.cms.gov/medicare/provider-enrollment-and-certification/guidanceforlawsandregulations/downloads/esrdpgmguidance.pdf↩︎
Ibid.↩︎
Medical Education Institute. About KDQOL Complete. https://www.kdqol-complete.org/about↩︎
Mapes DL, Lopes AA, Satayathum S et al. Health-related quality of life as a predictor of mortality and hospitalization: The Dialysis Outcomes and Practice Patterns Study (DOPPS). Kidney Int, 2003, 64:339-349. https://www.kidney-international.org/action/showPdf?pii=S0085-2538%2815%2949324-X↩︎
Medical Education Institute. KDQOL Complete Features. https://www.kdqol-complete.org/features
Comments