ESRD Network Reorganization and Home Dialysis: Changes & Challenges
Legislative History of ESRD Networks
On October 30, 1972 Section 2991 of Public Law 92-603 established the Medicare ESRD program that extended Medicare coverage to people with kidney failure who require dialysis or transplant to sustain their lives. On June 3, 1976, regulations were published that implemented this law and established 32 ESRD Network Organizations.
On June 13, 1978, Congress passed Public Law 95-292, requiring the Medicare ESRD program to encourage home dialysis and transplant and to be more cost effective while ensuring quality care and program accountability. It required ESRD Networks to have a coordinating council with representatives from each dialysis facility, an executive committee, and a medical review board. It required a patient to be on each network’s coordinating council and executive committee. That law listed these Network responsibilities:
"Encouraging, consistent with sound medical practice, the use of those treatment settings most compatible with the successful rehabilitation of the patient
Developing criteria and standards relating to the quality and appropriateness of patient care; and network goals with respect to the placement of patients in self-care settings and undergoing or preparing for transplantation
Evaluating the procedure by which facilities and providers in the network assess the appropriateness of patients for proposed treatment modalities
identifying facilities and providers that are not cooperating toward meeting network goals and assisting such facilities and providers in developing appropriate plans for correction
Submitting an annual report to the Secretary on July 1 of each year which shall include a full statement of the network's goals, data on the network's performance in meeting its goals (including data on the comparative performance of facilities and providers with respect to the identification and placement of suitable candidates in self-care settings and transplantation), identification of those facilities that have consistently failed to cooperate with network goals, and recommendations with respect to the need for additional or alternative services or facilities in the network in order to meet the network goals, including self-dialysis training, transplantation, and organ procurement facilities.”
 Section
9335 of Public
Law 99-509 reorganized the ESRD Networks, and required that
there be at least 17. This law added responsibility for
encouraging that “…patients who are suitable candidates for
vocational rehabilitation services be given access to such services and
encouraged to return to gainful employment.” It
established a registry with data collected “from network organizations,
transplant centers and other sources on all end stage renal disease
patients…” which became the United States Renal Data
System. It set funding for ESRD Networks by taking 50 cents per
HD treatment (adjusted for PD) from Medicare’s reimbursement to dialysis
facilities.
Section
9335 of Public
Law 99-509 reorganized the ESRD Networks, and required that
there be at least 17. This law added responsibility for
encouraging that “…patients who are suitable candidates for
vocational rehabilitation services be given access to such services and
encouraged to return to gainful employment.” It
established a registry with data collected “from network organizations,
transplant centers and other sources on all end stage renal disease
patients…” which became the United States Renal Data
System. It set funding for ESRD Networks by taking 50 cents per
HD treatment (adjusted for PD) from Medicare’s reimbursement to dialysis
facilities.
Today there are 18 ESRD Networks that contract with the Centers for Medicare & Medicaid Services. They serve all the facilities and patients within a geographic area. All of the ESRD Networks and the Quality Improvement Organizations (QIOS) that oversee them are nonprofits. All of the Networks are also members of the nonprofit Forum of ESRD Networks. The Forum advocates for ESRD Networks and coordinates projects and activities.
Changes & Challenges
Over the years, there have
been many changes in the ESRD Network program. In the past, some ESRD
Networks served facilities and patients in one state while others served
facilities and patients in multiple states and U.S. territories.
On May 1, 2026, CMS announced the winners of new 5-year
contracts (2026-2031). 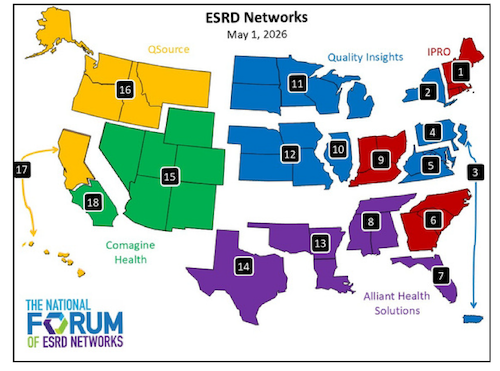 Those applying for ESRD Network
contracts expected to hear sooner, but they learned who had won
contracts and which Networks their contract included a few days earlier.
Though the transition to cover new territories is challenging, each of
these organizations has experience with oversight of ESRD Networks.
Those applying for ESRD Network
contracts expected to hear sooner, but they learned who had won
contracts and which Networks their contract included a few days earlier.
Though the transition to cover new territories is challenging, each of
these organizations has experience with oversight of ESRD Networks.
Today 5 entities—Alliant Health Solutions, Comagine Health, IPRO, QSource, and Quality Insights—have CMS contracts for the 18 ESRD Networks. Here’s a map of the Networks in the new contracts and the entities under which they operate as published in YOUR VOICE, YOUR HEALTH: A KIDNEY COMMUNITY NEWSLETTER, June 2026 (Special Edition).
According to the June 2026 KPAC Newsletter:
“Under the new contract, ESRD Networks will help increase awareness of treatment options such as home dialysis and kidney transplantation so patients can make informed choices that fit their goals and lifestyles. Efforts will also focus on improving care coordination, reducing avoidable hospitalizations and emergency room visits, and supporting smoother transitions between healthcare settings.
In addition, the Networks will promote whole-person health by supporting mental health screening and follow-up care, increasing nutrition awareness, encouraging preventive health measures, and helping patients stay active in their families, communities, and workplaces whenever possible.”
The following are key priorities and goals in the new contract:
2026-2031 Activities for ESRD Network Organizations
Empowering Patient and Family Choice by:
Encouraging modality & setting education to enable patients to make more informed decisions about treatment – Goal: to increase the percentage of patients who start or transition to home dialysis within the year by 5%.
Making transplant referrals easier and waitlisting more efficient as well as improving pre-transplant preparation – Goal: to increase the percentage of patients offered a transplant referral 14% and those accepting a higher risk kidney (KDPI >60) 10%.
Promoting Decision Making and Care Coordination by:
Improving patients’ access to care.
Increasing care coordination to help patients stay healthy and get “the right care at the right time in the right place, preventing crises before they happen.”– Goal: reduce unnecessary ER visits and inpatient hospitalizations by 10% each.
Focusing on Whole Health by:
Promoting physical health – Goal: to increase vaccine-eligible patients who get the flu vaccine to no less than 85%; increasing those getting the pneumonia vaccine by 15%.
Promoting mental health – Goal: screening no fewer than 95% of patients for depression and providing follow-up to 95% of patients who screen positive.
Increasing nutrition awareness – no specific goals mentioned.
Supporting patients’ work goals – no specific goals mentioned.
Enhancing Interoperability
Using Electronic Health Records to improve patients’ access to their data and improve efficiency of facilities’ workflow and use of real-time data – Goal: to increase dialysis facilities’ advanced electronic health record (EHR) use by 5%.
Supporting data accuracy and reporting in the End Stage Renal Disease Quality Reporting System (EQRS) and Quality Incentive Program (QIP) – Goal: “to create a more connected healthcare system where patient information flows seamlessly between dialysis centers, doctors, and patients themselves, making care safer and more efficient.”
ESRD Network Organization Reports to the Health and Human Services Secretary
By July 1 annually, Network Organizations are required to submit an annual report to the Secretary that includes:
A full statement of the Network’s goals & data on how well it met those goals.
Dialysis facilities that consistently did not cooperate with Network goals.
Recommendations for what is needed (more or different facilities or services) to meet Network goals, including self-dialysis training, transplantation, and organ procurement facilities.
ESRD Network Contact Emails (see map for states)
Networks 1, 6, 9 – ESRDNetworkProgram@ipro.org
Networks 2, 3, 4, 5, 10, 11, 12 – ESRDNetworks@qualityinsights.org
Networks 7, 8, 13, 14 – esrdinfo@allianthealth.org
Networks 15, 18 – esrdnetworks@comagine.org
Networks 16, 17 – esrdnetworks@qsource.org
KHARES (Kidney Health Analytics and Responsive Emergency Support) — KHARES@ipro.org
Conclusion
I’m supportive of the ESRD Network program’s goals, objectives and measures, especially related to patient choice of modality, encouraging home dialysis and vocational rehabilitation. I suspect that this 2026 reorganization has been stressful for everyone. The five entities that won contracts for ESRD Networks have not all covered the states they have now and will need time to get to know the facilities and patients. And patients and staff at dialysis facilities will need time get to know new ESRD Network staff. I call on patients receiving treatment at dialysis facilities and staff working in them to give grace to Network staff. To quote the June KPAC Newsletter about ESRD Networks, “No matter how the contracts change, one thing remains constant: Patients always come first.”
Comments