Anemia, EPO, Kidney Failure, and You
If you’re on dialysis, you most likely have anemia — a shortage of red blood cells. And, you may take EPO to treat it. Studies have led to a warning by the Food and Drug Administration (FDA) about EPO. Don’t panic! Read on, and we’ll tell you what this warning means to you.
Why You Need Anemia Treatment
Red blood cells carry oxygen to your body's cells. Anemia starves your cells of oxygen. This causes symptoms like:
- Severe fatigue
- Muscle weakness
- Shortness of breath
- Feeling cold all the time
- Pale skin, lips, gums, and nails
- Dizziness
- Trouble focusing your mind
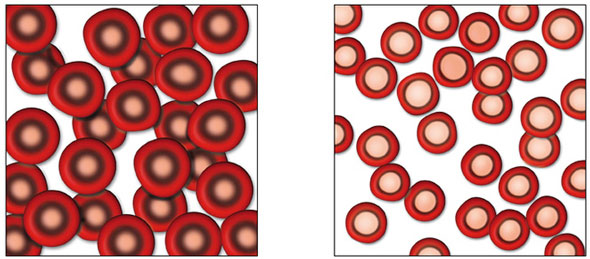
Left: Normal Red Blood Cells Right: Anemia
These symptoms are hard to deal with. People with anemia say things like:
"Even walking from the bedroom to the kitchen I rest after every two or three steps. I stop, because I don't have the strength to walk with. My quality of life has dropped so much that it's almost unbearable. I can't do anything to help my wife."1
Some have even quit their jobs—too tired to work—then later found out anemia could be treated.
In the long run, anemia can damage your heart. When there is less oxygen in your blood, your heart speeds up. Beating fast all the time makes your heart work much harder. The muscle of the main pumping chamber can become thick and overgrown(left ventricular hypertrophy, or LVH). LVH can make your heart so stiff it can't pump as well. LVH can cause heart failure. 2 It is vital to treat anemia.
How Anemia is Treated
In kidney failure, the main cause of anemia is a loss of erythropoietin (EPO). Kidneys sense how much oxygen is in your blood. When levels drop, they send out EPO. This hormone tells your bone marrow to make more red blood cells. As kidneys fail, they make less EPO—so you make fewer red blood cells. One part of treatment for anemia due to kidney failure is EPO. Three drugs on the market are
erythrocyte
(red blood cell)
stimulating agents
(ESAs), or cloned forms of EPO:
One part of treatment for anemia due to kidney failure is EPO. Three drugs on the market are
erythrocyte
(red blood cell)
stimulating agents
(ESAs), or cloned forms of EPO:
- Epogen®
- (epoetin alfa, Amgen)
- Aranesp®
- (darbepoetin alfa, Amgen)
- Procrit®
- (epoetin alfa, Ortho Biotech)
Epogen and Procrit are the same drug. Procrit is used in predialysis. Aranesp is a new form of EPO that lasts longer. It can be used at any stage of kidney disease. All three drugs treat other causes of anemia as well.
Iron is also needed to treat anemia; it is the building block the body uses to form new red blood cells. Iron works best when it is given through a vein.
Anemia Treatment Goals in Dialysis

Each month, you have a blood test for hemoglobin (Hb or Hgb). Hb picks up oxygen in your lungs and brings it to all of your cells. In healthy women, a normal Hb is 12.1 to 15.1 grams per deciliter (g/dL); in men, 13.8 to 17.2 g/dL. ("Normal" levels vary by lab.)
In people on dialysis, the Hb targets are below normal: 12 g/dL or greater in women and men. In fact, there is no lower limit now. 3 Hb levels are now dropping so low that many people with kidney failure need blood transfusions. 4
 Blood transfusions can be risky when you have kidney disease, for a number of reasons:
Blood transfusions can be risky when you have kidney disease, for a number of reasons:
- Extra fluid
- Extra potassium
- Blood borne illness (they can't screen for all disease)
- Antibodies that could make it harder for you to get a transplant
FDA Black Box Warnings
The FDA issues a black box warning when research suggests that a drug may cause harm in some cases. A black box warning was placed on all ESAs in March, 2007, due to new research. None of the new studies were of people on dialysis.
In people with cancer, four new studies found problems when EPO was used:
- A number of studies have linked anemia with poor outcomes in people with head and neck cancers. 5,6,7,8 But in a Danish study, patients given EPO to reach a (normal) Hb target of 14 to 15.5 g/dL did worse than those who took a placebo.
- A study of cancer patients not on chemo found that EPO did not reduce the need for transfusions (the target Hb was 12 g/dL). Patients who took EPO were also more likely to die. 9
- A study of whether EPO would improve quality of life in people with non-small cell lung cancer was stopped early. More people in the EPO group died than those who took a placebo. Target Hb was 12 to 14 g/dL.
- Hoffman-La Roche was testing a new ESA in people with non-small cell lung cancer (Hb target of 11 to 13 g/dL). Those who took the drug were more likely to die. The study was stopped early.
The FDA also looked at two studies in chronic kidney disease (CKD) before dialysis:
- The CHOIR study found that patients in a higher Hb group (target of 13.5 g/dL) had more heart problems, hospital stays, or death than those in a lower Hb group (target of 11.3 g/dL). 10
- The CREATE study failed to show that full correction of anemia in CKD (target of 13 to 15 g/dL) would prevent heart damage. This study used epoetin beta, a drug that is not sold in the U.S. 11
EPO and Quality of Life

Your day to day quality of life may affect you more than a risk of a poor outcome. Research has shown that people on dialysis feel much better when their anemia is treated with EPO.12,13,14,15The FDA does not believe the measures of quality of life are accurate, and does not count these studies.
But, a 48-72 week long Swedish study randomly assigned 416 people (predialysis, on hemodialysis, or on peritoneal dialysis) to one of two Hb groups:
- A target Hb of 13.5 to 16 g/dL
- A target Hb of 9 to 12 g/dL
This study found no higher risk of adverse events or death. The higher Hb group had better quality of life. 16
In Japan, a study was done with 322 people. 17 Those who took part had kidney disease and Hbs less than 10, but were not yet on dialysis. They were randomly assigned to get iron and ESA’s to bring them to:
- A high Hb (11-13 g/dL)
- A low Hb (9-11 g/dL)
After 48 weeks, the rate of adverse events was the same in both groups. Quality of life was much better in the high Hb group. The high Hb group also had much less LVH.
What You Should Do
Take an ESA if your doctor prescribes it. The risk of anemia is far greater than the risk of the drug when it is used according to current guidelines. On the Black Box Warning, the FDA suggests using the lowest dose that will help you avoid transfusions. Your blood iron levels need to be in the target range so you have the building blocks to make red blood cells. This will let your EPO work.
Inflammation from an infection can also keep your body from using EPO. This is called EPO resistance. Tell your care team about fever, swelling, redness in your access, or other illness so it can be treated. This can help you need less EPO.
Getting more dialysis helps the red blood cells you do have to live longer. This means you may need less EPO to have a Hb in the target range. One study found less LVH and less EPO resistance in patients on short daily hemodialysis (HD). 18 A number of studies have also found that less EPO is needed for short daily 19,20,21,22 or for extended (nocturnal) 23,24,25,26 HD.
Talk with Your Doctor
EPO has been safely used to keep people on dialysis in a target Hb range of 11 to 12 g/dL for nearly 20 years— since 1989.
The Renal Physician's Association says that you and your doctor should decide how to treat your anemia. 27
You are the only one who can decide what you value more: your quality of life, or the chance of a risk. If there is a tradeoff to be made, you are the only one who can make it. Talk with your doctor and decide what will be best for you.
References:
- Schatell D, Witten B. Anemia: Dialysis Patients' Experiences. Nephrol News Issues. 200
- Zalunardo N, Levin A. Anemia and the heart in chronic kidney disease. Semin Nephrol. 2006 Jul;26(4):290-5
- CMS RAISES DIALYSIS REIMBURSEMENT FOR 2012, REVISES QIP Renal Business Today.
- Unintended Consequence for Dialysis Patients as Drug Rule Changes The New York Times.
- Prosnitz RG, Yao B, Farrell CL, Clough R, Brizel DM. Pretreatment anemia is correlated with the reduced effectiveness of radiation and concurrent chemotherapy in advanced head and neck cancer. Int J Radiat Oncol Biol Phys. 2005 Mar 15;61(4):1087-95
- Stadler P, Putnik K, Kreimeyer T, Sprague LD, Koelbl O, Schafer C. Split course hyperfractionated accelerated radio-chemotherapy (SCHARC) for patients with advanced head and neck cancer: influence of protocol deviations and hemoglobin on overall survival, a retrospective analysis. BMC Cancer. 2006 Dec 7;6:279
- Zhao KL, Liu G, Jiang GL, Wang Y, Zhong LJ, Wang Y, Yao WQ, Guo XM, Wu GD, Zhu LX, Shi XH. Association of haemoglobin level with morbidity and mortality of patients with locally advanced oesophageal carcinoma undergoing radiotherapy—a secondary analysis of three consecutive clinical phase III trials. Clin Oncol (R Coll Radiol). 2006 Oct;18(8)621-7
- van de Pol SM, Doornaert PA, de Bree R, Leemans CR, Slotman BJ, Langendijk JA. The significance of anemia in squamous cell head and neck cancer treated with surgery and postoperative radiotherapy. Oral Oncol. 2006 Feb;42(2):131-8
- "Dear Health Care Professional" letter. Not yet published.
- Singh AK, Szczech L, Tang KL, Barnhart H, Sapp S, Wolfson M, Reddan D. Correction of anemia with epoetin alfa in chronic kidney disease. N Engl J Med. 2006 Nov 16;355(20):2085-98
- Drueke TB, Locatelli F, Clyne N, Eckardt KU, Macdougall IC, Tsakiris D, Burger HU, Scherhag A. Normalization of hemoglobin level in patients with chronic kidney disease and anemia. N Engl J Med. 2006 Nov 16;355(20):2071-84
- Delano BG. Improvements in quality of life following treatment with r-HuEPO in anemic hemodialysis patients. Am J Kidney Dis. 1989 Aug;14(2 Suppl):14-8
- Stevens JM, Auer J, Strong CA, Hughes RT, Oliver DO, Winearis CG, Cotes PM. Stepwise correction of anaemia by subcutaneous administration of human recombinant erythropoietin in patients with chronic renal failure maintained by continuous ambulatory peritoneal dialysis. Nephrol Dial Transplant. 1991;6(7):487-94
- Levin NW, Lazarus JM, Nissenson AR. National Cooperative rHu Erythropoietin Study in patients with chronic renal failure—an interim report. Am J Kidney Dis. 1993 Aug;22(2 Suppl 1):3-12
- Glaspy J. Phase III clinical trials with darbepoetin: implications for clinicians. Best Pract Res Clin Haematol. 2005;18(3):407-16
- Furuland H, Linde T, Ahlmen J, Christensson A, Strombom U, Danielson BG. A randomized controlled trial of haemoglobin normalization with epoetin alfa in pre-dialysis and dialysis patients. Nephrol Dial Transplant. 2003 Feb;18(2):353-61
- Akizawa T, Gejyo F, Nishi S, Iino Y, Watanabe Y, Suzuki M, Saito A, Akiba T, Hirakata H, Fukuhara S, Morita S, Hiroe M, Hada Y, Suzuki M, Akaishi M, Iwasaki M, Tsubakihara Y, and the KRN321 STUDY Group. Positive outcomes of high hemoglobin target in patients with chronic kidney disease not on dialysis: a randomized controlled study. Therap Apheresis and Dial. 2011;15(5):431-440
- Ayus JC, Mizani MR, Achinger SG, Thadhani R, Go AS, Lee S. Effects of short daily versus conventional hemodialysis on left ventricular hypertrophy and inflammatory markers: a prospective, controlled study. J Am Soc Nephrol. 2005 Sep;16(9):2778-88
- Ting GO, Kjellstrand C, Freitas T, Carrie BJ, Zarhamee S. Long-term study of high-comorobidity ESRD patients converted from conventional to short daily hemodialysis. Am J Kidney Dis. 2003 Nov;42(5):1020-35
- Koshikawa S, Akizawa T, Saito A, Kurokawa K. Clinical effect of short daily in-center hemodialysis. Nephron Clin Pract. 2003;95(1):c23-30
- Ettari G, Boccardo G, De Prisco O, Maurino D. [Daily short dialysis. First results in a group of patients in home dialysis training] article in Italian. Minerva Urol Nefrol. 2002 Jun;54(2):139-43
- Vos PF, Zilch O, Kooistra MP. Clinical outcome of daily dialysis. Am J Kidney Dis. 2001 Jan;37(1 Suppl 2):S99-S102
- Klarenbach S, Heidenheim AP, Leitch R, Lindsay RM. Reduced requirement for erythropoietin with quotidian hemodialysis therapy. ASAIO J. 2002 Jan-Feb;48(1):57-61
- Agar JW, Knight RJ, Simmonds RE, Boddington JM, Waldron CM, Somerville CA. Nocturnal haemodialysis: an Australian cost comparison with conventional satellite haemodialysis. Nephrology (Carlton). 2005 Dec;10(6):557-70
- Yuen D, Richardson RM, Fenton SS, McGrath-Chong ME, Chan CT. Quotidian nocturnal hemodialysis improves cytokine profile and enhances erythropoietin responsiveness. ASAIO J. 2005 May-Jun;51(3):236-41
- Schwartz DI, Pierratos A, Richardson RM, Fenton SS, Chan CT. Impact of nocturnal home hemodialysis on anemia management in patients with end-stage renal disease. Clin Nephrol. 2005 Mar;63(3):202-8
- RPA Guidance to Nephrology Care Providers Regarding the FDA Public Health Advisory on ESAs. (accessed 3/18/07)