LVH: Heading Off a Common Heart Problem
As the old song goes, "the knee bone's connected to the leg bone...." Kidney failure affects your whole body, and your heart can be first in line for harm. We'll tell you how to prevent it (hint: home dialysis can help!), what tests to ask about, and how to protect your heart.
The heart is a lonely pumper
 Your heart pumps your blood through a 100,000 mile loop of blood vessels, 80 times or so per minute, 24 hours a day. That's about 42 million beats a year.
Your heart pumps your blood through a 100,000 mile loop of blood vessels, 80 times or so per minute, 24 hours a day. That's about 42 million beats a year.
Four chambers make this happen—two atria take blood in from your veins, and two ventricles pump it out through your arteries to your lungs and the rest of your body. Valves are doors that keep the blood from backing up. (In fact, the "lub-dub" sound of a heartbeat is heard when your valves open and close.)
Meet the problem: LVH
A common heart problem in people on dialysis occurs when the muscle of the main pumping chamber grows too thick. This is left ventricular hypertrophy (LVH). LVH can make your heart stiff and take up space that is needed for blood. This can lead to slow heart failure—or sudden death. A study that tracked in-center hemodialysis (HD) patients for 10 years found that LVH was the strongest predictor of sudden death. 1
From 16.4% 2 to 75.9% 3 of people on dialysis have LVH—which starts early in kidney disease. 4 Diabetes adds to the problem; with it, the function of the left ventricle is not as strong, even when the degree of LVH is the same. 5
How to prevent LVH
The main cause of LVH on dialysis is too much fluid, which leads to high blood pressure. 6 Inside the body, water is in three "compartments":
- Inside your cells
- Between your cells
- In your bloodstream
Dialysis can only remove water that is in your bloodstream—but 2/3 of your body water is inside your cells. So, if you gain a lot of water, standard hemodialysis (HD) done three times a week can't remove it all. This can cause high blood pressure and LVH.
On PD, keeping blood pressure normal and eating less salt help LVH. 7 On standard HD, sodium modeling can reduce symptoms—but it also leaves your body with extra salt, so you are thirsty and may gain more water weight. 8 You can help prevent LVH by eating a low salt diet and limiting fluid weight gain between treatments.
Daily and nocturnal HD can help
Stiff, calcified arteries 9 or too much beta-2 microglobulin 10 (which also leads to joint damage) can add to LVH. These problems improve with longer or more-frequent HD. Daily and nocturnal HD remove more water from the bloodstream and from inside cells; these treatments can help prevent (or treat) LVH. In a year-long study, both options helped reduce left ventricular mass more than in-center HD. 11
Patients who switched to daily HD with the same dialysis adequacy (Kt/V) had less fluid between their cells, lower blood pressure, and lower left ventricular mass than when they did standard HD, and high-risk patients who switched to daily HD had less left ventricular mass—and lots of other pluses, like higher albumin levels, better bone health, less pain, more energy, and better physical function. 12
Nocturnal HD has improved LVH in patients with known heart problems. 13 The treatment helped make patients' arteries less stiff so they respond as they should to stress. 14 Compared to patients who stayed on in-center treatment three times per week, those who switched to nocturnal HD had less LVH and lower blood pressure. 15
Do you have LVH?
The good news is that LVH can be reversed. 3 If you don't have it, you can help prevent it. And if you do have it, you can take steps to improve your heart health. Ask your doctor about getting tested for LVH—you can have it with no symptoms (or you may be short of breath, dizzy, or have chest pain). Research has found a number of tests that can check for the problem.
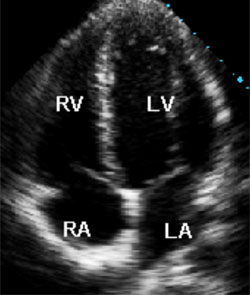
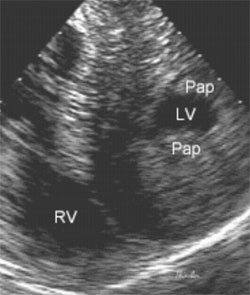
- Echocardiogram
- an "echo" uses painless sound waves to show your pumping chambers and valves. It will reveal the size and function of your left ventricle (see figures 1 and 2 below), which can predict future problems. 16
- 24-hour blood pressure (BP)
- with a small machine on your belt and a cuff on your arm, your BP can be checked all day and night. This tells your doctor much more than a single check. If your BP is high all the time 2,17,18,19 or does not drop at night 20 (it should), you are at risk for heart problems.
- Bioimpedance analysis (BIA)
- checks for fluid overload by looking for water in and outside of your cells. The technique, which uses sensors placed on your head and neck (Bio-Z), is painless and not invasive. BIA predicts LVH on dialysis. 21
- C-reactive protein (CRP)
- a CRP blood test measures inflammation, which has been linked to heart damage in people on dialysis. 22,23 Even one high CRP test level can predict heart risk in people on PD. 24
- Cardiac troponin T (CTnT)
- a blood test that is a marker for damage to the heart muscle itself. It adds value to an echo and has been shown to predict results in people on dialysis in research. 25,26,27
- Tumor necrosis factor alpha (TNF-alpha)
- a group of proteins that tell cells when to die. In a study, this test was able to predict LVH in people on dialysis. 28 (It is not yet being used for this purpose in routine practice.)
|
|
| Figure 1: Normal echocardiogram (left ventricle at LV) | Figure 2: Echocardiogram showing severe LVH |
Treatment for LVH
If you have LVH, some things you can do include:
- Quit smoking.
- Tobacco use has been found to raise the risk of LVH by 42%. 2 If you smoke, stopping can help protect your heart. Can't do it alone? Ask your doctor about prescription drugs to help you.
- Eat enough protein.
- Low serum albumin levels seem to make LVH progress faster. 2,29,30 If you can't face protein, you may not be getting enough dialysis to keep up your appetite. Getting more treatment can help your heart.
- Ask about angiotensin receptor blockers (ARBs) and angiotensin-converting enzyme (ACE) inhibitors.
- Some blood pressure drugs in these two classes have reversed LVH, including losartan (25% less LVH vs. placebo or other drugs)31,32, losartan plus enalapril (an extra 28% less LVH)33, valsartan 34, and imidapril 35.
- Get bone disease treated.
- Having too much parathyroid hormone 2 and/or not enough active vitamin D (calcitriol) makes LVH worse. Taking calcitriol has been shown to improve it, 36,37 so you can do both your bones and your heart a favor at the same time.
Conclusion
While LVH is quite common, it does not have to happen. There is much you can do to prevent LVH, slow it down, or even make it better. Talk with your doctor about tests for LVH so you know how your heart is doing. Ask how often these tests should be done.
If you have LVH, talk with your doctor about a treatment plan. You may also want to ask to see a heart specialist (cardiologist) to be sure that you get the help you need to feel your best.
References:
- Paoletti E, Specchia C, Di Maio G, Bellino D, Damasio B, Cassottana P, Cannella G. The worsening of left ventricular hypertrophy is the strongest predictor of sudden cardiac death in haemodialysis patients: a 10 year survey. Nephrol Dial Transplant. 2004 Jul;19(7):1829-34.
- Stack AG, Saran R. Clinical correlates and mortality impact of left ventricular hypertrophy among new ESRD patients in the United States. Am J Kidney Dis. 2002 Dec;40(6):1202-10.
- Kutlay S, Dincer I, Sengul S, Nergizoglu G, Duman N, Erturk S. The long-term behavior and predictors of left ventricular hypertrophy in hemodialysis patients. Am J Kidney Dis. 2006 Mar;47(3):485-92.
- Paoletti E, Bellino D, Cassottana P, Rolla D, Cannella G. Left ventricular hypertrophy in nondiabetic predialysis CKD. Am J Kidney Dis. 2005 Aug;46(2):320-7 Comment in: Am J Kidney Dis. 2005 Dec;46(6):1148; author reply 1148-9.
- Miyazato J, Horio T, Takiuchi S, Kamide K, Sasaki O, Nakamura S, Nakahama H, Inenaga T, Takishita S, Kawano Y. Left ventricular diastolic dysfunction in patients with chronic renal failure: impact of diabetes mellitus. Diabet Med. 2005 Jun;22(6):730-6.
- Koc M, Toprak A, Tezcan H, Bihorac A, Akoglu E, Ozener IC. Uncontrolled hypertension due to volume overload contributes to higher left ventricular mass index in CAPD patients. Nephrol Dial Transplant. 2002 Sep;17(9):1661-6.
- Asci G, Ozkahya M, Duman S, Toz H, Erten S, Ok E. Volume control associated with better cardiac function in long-term peritoneal dialysis patients. Perit Dial Int. 2006 Jan-Feb;26(1):85-8. Comment in: Perit Dial Int. 2006 Jan-Feb;26(1):49-52.
- Akcahuseyin E, Nette RW, Vincent HH, van Duyl WA, Krepel H, Weimar W, Zietse R. Simulation study of the intercompartmental fluid shifts during hemodialysis. ASAIO J. 2000 Jan-Feb;46(1):81-94.
- Nitta K, Akiba T, Uchida K, Otsubo S, Otsubo Y, Takei T, Ogawa T, Yumura W, Kabaya T, Nihei H. Left ventricular hypertrophy is associated with arterial stiffness and vascular calcification in hemodialysis patients. Hypertens Res. 2004 Jan;27(1):47-52.
- Zumrutdal A, Sezer S, Demircan S, Seydaoglu G, Ozdemir FN, Haberal M. Cardiac troponin I and beta 2 microglobulin as risk factors for early-onset atherosclerosis in patients on haemodialysis. Nephrology (Carlton). 2005 Oct;10(5):453-8.
- Weinreich T, De los Rios T, Gauly A, Passlick-Deetjen J. Effects of an increase in time vs. frequency on cardiovascular parameters in chronic hemodialysis patients. Clin Nephrol. 2006 Dec;66(6):433-9.
- Fagugli RM, Reboldi G, Quintaliani G, Pasini P, Ciao G, Cicconi B, Pasticci F, Kaufman JM, Buoncristiani U. Short daily hemodialysis: blood pressure control and left ventricular mass reduction in hypertensive hemodialysis patients. Am J Kidney Dis. 2001 Aug;38(2):371-6.
- Chan C, Floras JS, Miller JA, Pierratos A. Improvement in ejection fraction by nocturnal haemodialysis in end-stage renal failure patients with coexisting heart failure. Nephrol Dial Transplant. 2002 Aug;17(8):1518-21.
- Chan CT, Jain V, Picton P, Pierratos A, Floras JS. Nocturnal hemodialysis increases arterial baroreflex sensitivity and compliance and normalizes blood pressure of hypertensive patients with end-stage renal disease. Kidney Int. 2005 Jul;68(1):338-44.
- Chan CT, Floras JS, Miller JA, Richardson RM, Pierratos A. Regression of left ventricular hypertrophy after conversion to nocturnal hemodialysis. Kidney Int. 2002 Jun;61(6):2235-9.
- Zoccali C, Benedetto FA, Mallamaci F, Tripepi G, Giacone G, Cataliotti A, Seminara G, Stancanelli B, Malatino LS. Prognostic value of echocardiographic indicators of left ventricular systolic function in asymptomatic dialysis patients. J Am Soc Nephrol. 2004 Apr;15(4):1029-37.
- Nakazato T, Kawada T, Shigematsu T, Yamada K. Left ventricular hypertrophy was infrequent in patients starting dialysis after undergoing a strict blood pressure control in the pre-dialytic period. Intern Med. 2002 Nov;41(11):925-30.
- Cannella G, Paoletti E, Ravera G, Cassottana P, Araghi P, Mulas D, Peloso G, Delfino R, Messa P. Inadequate diagnosis and therapy of arterial hypertension as causes of left ventricular hypertrophy in uremic dialysis patients. Kidney Int. 2000 Jul;58(1):260-8.
- Chan CT, Jain V, Picton P, Pierratos A, Floras JS. Nocturnal hemodialysis increases arterial baroreflex sensitivity and compliance and normalizes blood pressure of hypertensive patients with end-stage renal disease. Kidney Int. 2005 Jul;68(1):338-44.
- Fagugli RM, Quintaliani G, Pasini P, Ciao G, Cicconi B, Pasticci F, Buoncristiani U. Blunted nocturnal blood pressure decrease and left-ventricular mass in hypertensive hemodialysis patients. Nephron. 2002 May;91(1):79-85.
- Fagugli RM, Pasini P, Quintaliani G, Pasticci F, Ciao G, Cicconi B, Ricciardi D, Santirosi PV, Buoncristiani E, Timio F, Valente F, Buoncristiani U. Association between extracellular water, left ventricular mass and hypertension in haemodialysis patients. Nephrol Dial Transplant. 2003 Nov;18(11):2332-8.
- London GM, Marchais SJ, Guerin AP, Metivier F, Adda H, Pannier B. Inflammation, arteriosclerosis, and cardiovascular therapy in hemodialysis patients. Kidney Int Suppl. 2003 May;(84):S88-93.
- Zumrutdal A, Sezer S, Demircan S, Seydaoglu G, Ozdemir FN, Haberal M. Cardiac troponin I and beta 2 microglobulin as risk factors for early-onset atherosclerosis in patients on haemodialysis. Nephrology (Carlton). 2005 Oct;10(5):453-8.
- Wang AY, Woo J, Lam CW, Wang M, Sea MM, Lui SF, Li PK, Sanderson J. Is a single time point C-reactive protein predictive of outcome in peritoneal dialysis patients? J Am Soc Nephrol. 2003 Jul;14(7):1871-9.
- Wang AY, Lam CW, Yu CM, Wang M, Chan IH, Lui SF, Sanderson JE. Troponin T, left ventricular mass, and function are excellent predictors of cardiovascular congestion in peritoneal dialysis. Kidney Int. 2006 Aug;70(3):444-52. Comment in: Kidney Int. 2006 Aug;70(3):408-10.
- Wang AY, Lam CW, Wang M, Chan IH, Goggins WB, Yu CM, Lui SF, Sanderson JE. Prognostic Value of Cardiac Troponin T Is Independent of Inflammation, Residual Renal Function, and Cardiac Hypertrophy and Dysfunction in Peritoneal Dialysis Patients. Clin Chem. 2007 Mar 29; [Epub ahead of print]
- Duman D, Tokay S, Toprak A, Duman D, Oktay A, Ozener IC, Unay O. Elevated cardiac troponin T is associated with increased left ventricular mass index and predicts mortality in continuous ambulatory peritoneal dialysis patients. Nephrol Dial Transplant. 2005 May;20(5):962-7. Erratum in: Nephrol Dial Transplant. 2005 Aug;20(8):1773. Unay, Ozlem [added].
- Erten Y, Tulmac M, Derici U, Pasaoglu H, Altok Reis K, Bali M, Arinsoy T, Cengel A, Sindel S. An association between inflammatory state and left ventricular hypertrophy in hemodialysis patients. Ren Fail. 2005;27(5):581-9.
- Moon KH, Song IS, Yang WS, Shin YT, Kim SB, Song JK, Park JS. Hypoalbuminemia as a risk factor for progressive left-ventricular hypertrophy in hemodialysis patients. Am J Nephrol. 2000 Sep-Oct;20(5):396-401.
- Nasri H, Baradaran A, Naderi AS. Close association between parathyroid hormone and left ventricular function and structure in end-stage renal failure patients under maintenance hemodialysis. Acta Med Austriaca. 2004 Aug;31(3):67-72.
- Shibasaki Y, Masaki H, Nishiue T, Nishikawa M, Matsubara H, Iwasaka T. Angiotensin II type 1 receptor antagonist, losartan, causes regression of left ventricular hypertrophy in end-stage renal disease. Nephron. 2002 Mar;90(3):256-61.
- Kanno Y, Kaneko K, Kaneko M, Kotaki S, Mimura T, Takane H, Suzuki H. Angiotensin receptor antagonist regresses left ventricular hypertrophy associated with diabetic nephropathy in dialysis patients. J Cardiovasc Pharmacol. 2004 Mar;43(3):380-6
- Suzuki H, Kanno Y, Kaneko K, Kaneko M, Kotaki S, Mimura T, Takane H. Comparison of the effects of angiotensin receptor antagonist, angiotensin converting enzyme inhibitor, and their combination on regression of left ventricular hypertrophy of diabetes type 2 patients on recent onset hemodialysis therapy. Ther Apher Dial. 2004 Aug;8(4):320-7.
- Suzuki H, Nakamoto H, Okada H, Sugahara S, Kanno Y. A selective angiotensin receptor antagonist, Valsartan, produced regression of left ventricular hypertrophy associated with a reduction of arterial stiffness. Adv Perit Dial. 2003;19:59-66.
- Matsumoto N, Ishimitsu T, Okamura A, Seta H, Takahashi M, Matsuoka H. Effects of imidapril on left ventricular mass in chronic hemodialysis patients. Hypertens Res. 2006 Apr;29(4):253-60.
- Kim HW, Park CW, Shin YS, Kim YS, Shin SJ, Kim YS, Choi EJ, Chang YS, Bang BK. Calcitriol regresses cardiac hypertrophy and QT dispersion in secondary hyperparathyroidism on hemodialysis. Nephron Clin Pract. 2006;102(1):c21-9.
- Park CW, Oh YS, Shin YS, Kim CM, Kim YS, Kim SY, Choi EJ, Chang YS, Bang BK. Intravenous calcitriol regresses myocardial hypertrophy in hemodialysis patients with secondary hyperparathyroidism. Am J Kidney Dis. 1999 Jan;33(1):73-81.