Fistula: Miracle and Thief

“Lifeline” is the popular term for the surgically modified blood vessel we call a fistula. The regular veins responsible for returning blood to our hearts are too thin-walled and delicate to withstand repeated needling or the speed of blood flow required for effective dialysis. Arteries could be suitable, but they lie too deeply under the skin to be easily reached for cannulation.
The creation of a fistula is a marvelous innovation—but there are consequences. Our systems run just perfectly when health is good, but small invasions/alterations cause imbalance. In constructing a fistula, some of the regular blood supply to the hand via an artery is rerouted to the vein that forms the fistula. In this sense the fistula ends up “stealing” some blood and the hand may suffer impoverished circulation. The diagrams illustrate fistula creation and subsequent development of the access.
Fig. 1. Sections of an artery and vein (e.g., in the lower arm) are used for fistula creation. Veins are closer to the skin’s surface than arteries and therefore more readily reached for cannulation. However, veins are thin-walled compared with arteries, and need to be strengthened for the rigours of dialysis. By creating increased pressure, blood volume and turbulence in the vein, it responds in turn by developing greater diameter and strength.
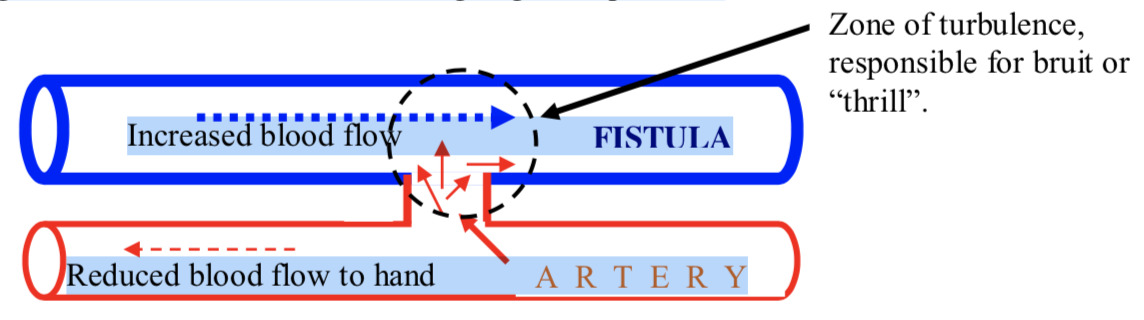
Fig.2. The surgery for creating the conditions that will modify the vein to a fistula involves creating a small connection—an anastomosis—between the vein and its associated artery. Since blood flow in the artery is faster and at greater pressure than in the vein, blood readily rushes through the anastomosis into the vein. Considerable turbulence at the junction causes the thrill (bruit) and this may be felt reverberating some way up the fistula. The increased stress on the walls of the vein stimulates it to develop greater strength and diameter following the weeks after surgery.
Fig 3. After 6 – 8 weeks the walls of the vein become thickened and sufficiently strengthened to accommodate regular cannulation and blood flowing at greater pressure.
Returning home after surgery, at the quietness of bedtime and without even holding the arm up to the ear, one may be astonished to hear a hissing/pulsing sound coming from the newly constructed fistula. While this is normal, in not many weeks the sound disappears under the layers of reinforcing tissue that develop. The feel of the thrill (bruit) remains.
 Improving Blood Flow to the Deprived Hand
Improving Blood Flow to the Deprived Hand
Dialysors often experience cold hands/numb fingers following fistula creation, and if one’s circulation before surgery was poor it will be exacerbated following surgery. This can be offset to a great degree through consistent hand exercises. For a great device look no further than sections cut from a pool noodle. They fit snugly into the palm of the hand, have great spring and resilience and may be deployed whilst out walking, watching TV or lying in bed. As with all exercise, consistency is the key and 20 minutes a day is recommended. Marked results may be noted within a few weeks.
Comments
Pui Pui
Jun 14, 2020 12:05 PM