Helpful Home Hemo Hacks

 Dialysis Machine and Setting Up
Dialysis Machine and Setting Up
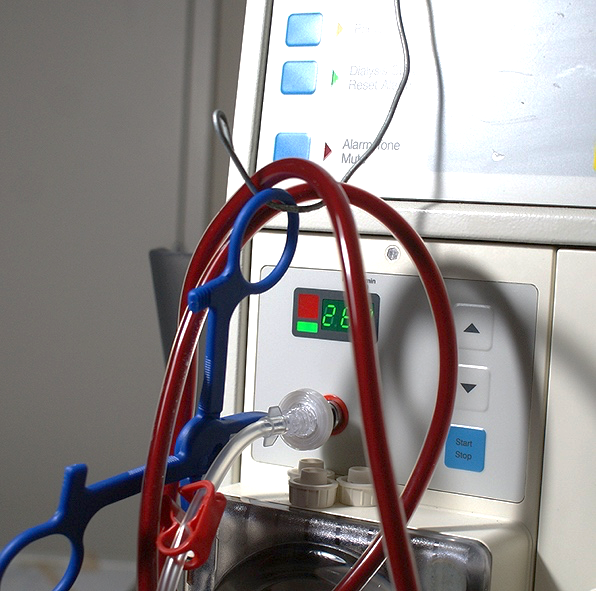
My machine is a Fresenius 4008B—which is no longer in production, yet widely used in Australia and New Zealand by home dialysors. Renowned for its reliability and ease of use, its drawback is size making it unsuitable for travel.
I have mine snugged up right next to my bed for convenience, and have attached a wire loop on which to hang the bloodlines (Figure 1). This keeps them clear of the floor, ensuring that they remain free of obstacles and the edge of the bed when I turn over.
Before each dialysis session, the machine is put through a 32-minute disinfection cycle. I use this time to attach the bloodlines, saline, and heparin. In addition, I prepare a needle tray with swabs, absorbent towel, heparin syringes, as well as the needles themselves by wrapping tape 360° round their hubs.
Next, the Fresenius goes through a cycle called “test” for 6 minutes. I use this time to disinfect the fistula, cannulate, stick the needles down and add saline and heparin to the arterial and venous needle tubes. “Prime” comes next and this is to fill all the lines with saline, ensuring the expulsion of air.
 Cannulation: Rope Ladder
Cannulation: Rope Ladder
Confidence in one’s needle position and security ensures relaxed dialysis. In-center, I noted the nurses slipping the tape (sticky side up) under the hub using both hands before crossing it over on each side to achieve the approved chevron fold. This is not easy single-handed for the solo dialysor—unless one pre-attaches the tape with a complete 360° turn around the needle hub (Figure 2). For such a method the wings get in the way, but they are designed to be easily twisted off. The figure also illustrates the use of Touch Cannulation (holding the needle by the tubing), and in my case, steadying the works by having my little finger propped against the fistula wall. An added benefit of Touch Cannulation is the clear view of the blood flashback as the needle tip progresses within the fistula lumen.
Figure 3 (below) shows the arterial needle in and the second arm of the chevron being stuck down. Tiny red spots below the needle indicate last week’s sticks, as I worked my way up the inner surface of the fistula. With the ladder technique, we are urged to utilize as much of the access as possible, thereby ensuring even development of healing (fibrous) tissue with no weak spots.

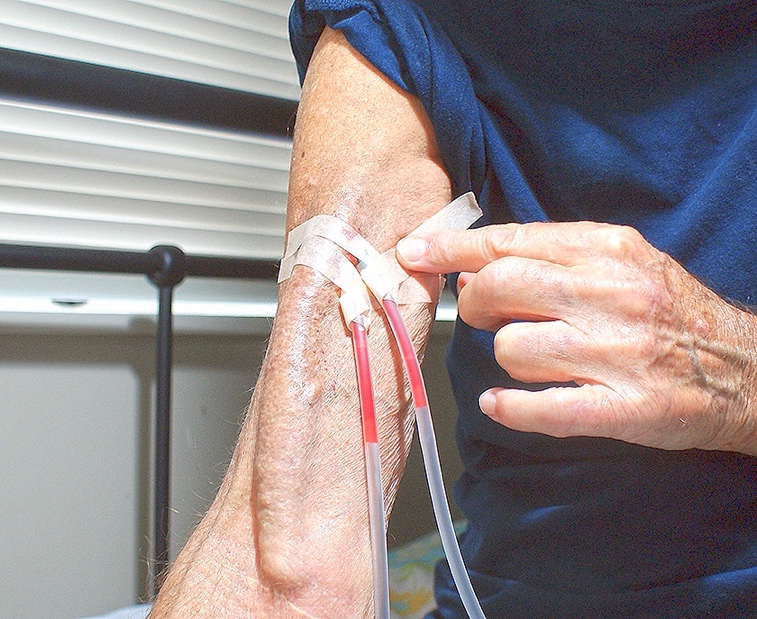 Figure 4: The venous needle is in and the tape secured. Further tape (far broader) will be used as a final “wrap around.” The system is secure, and in over 4 years of solo dialysis (touch wood!) I’ve not had a leakage or a dislodged needle.
Figure 4: The venous needle is in and the tape secured. Further tape (far broader) will be used as a final “wrap around.” The system is secure, and in over 4 years of solo dialysis (touch wood!) I’ve not had a leakage or a dislodged needle.
 At the close of dialysis, the task of unsticking the tape and holding ten minutes for each needle is tedious and frustrating. The tapes are extremely sticky and hang onto each other with tenacity. I use scissors to cut them free. (Figure 5). Note that the scissors are well ABOVE the needle tubes.
At the close of dialysis, the task of unsticking the tape and holding ten minutes for each needle is tedious and frustrating. The tapes are extremely sticky and hang onto each other with tenacity. I use scissors to cut them free. (Figure 5). Note that the scissors are well ABOVE the needle tubes.

The scissors are kept in chlorhexadine as disinfectant and also to prevent the tape from sticking to the blades, which makes cutting difficult. (Figure. 6)
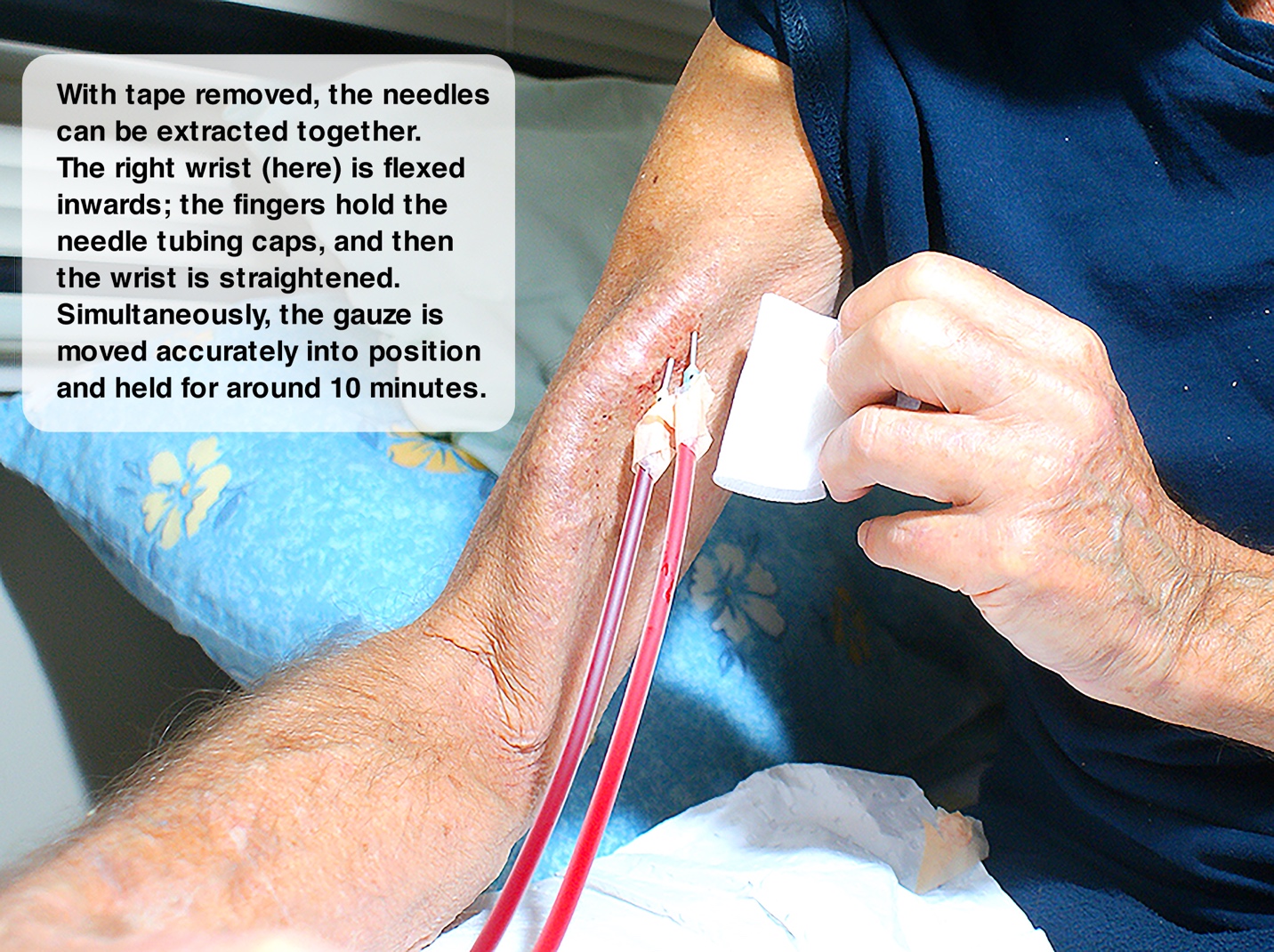
Figure 7. Once all the tapes are sufficiently cleared, the needles may be extracted simultaneously to halve the holding time. My right hand wrist is flexed inwards so that the needle caps may be held by my fingers. By straightening my wrist again, I apply pressure to the needle tubing. The needles pop out together and the gauze is held against the holes for 8 – 10 minutes. Having the needles close together allows one to treat the exit points as one. This makes for easy and efficient holding with one hand. In addition, if one is active during dialysis (working on craft, computer etc.), arm movement tends to act on the needles as one—minimizing uneven forces that could lead to infiltrations.
Provided blood flow in the fistula is adequate, there need be no concern about recirculation of returned blood with outgoing blood. Research indicates that the blood pump speed needs to be at least 100 ml/min slower than the blood flow speed in the fistula. As good fistulas typically support a flow of 500 – 1000 ml/min this would allow a pump speed of 400 m/min for a flow of 500 ml/min. (We should note that speeds above 350 ml/min are no longer recommended.) An investigation by Rothera et.al (2011) found by experiment that needles 2.5 cm apart did not result in any re-circulation between blood returning and blood being withdrawn. Moreover, Fresenius’s detailed instruction states 1.5 cm as minimum for needle spacing. 
Finally (Figure 8): many of us experience dialysis brain fog. This can be offset to a degree by keeping creatively active on work, projects, or other activities that demand concentration. Movies and web browsing are not as effective.
Comments
phyllis schiff
Oct 13, 2020 3:22 PM
Jacqueline Mordaunt
Oct 10, 2020 12:21 AM