Touch Cannulation: The Genius of Stuart Mott

Reposted with permission from HemoDoc, From Doctor to Patient, 2012
Many aspects of dialysis care that is beneficial for patients came about by serendipitous application of chance observations. The buttonhole technique came into practice when Dr. Twardowski had little option on some patients with only short areas on fistulas for cannulation. He began using a single site cannulation that developed scar tissue and a track. In the days before highly available access to disposable needles was the rule, multiple reuse of needles created dull points. After successfully establishing buttonhole or constant site cannulation, the observation that new sharp needles caused more difficulties than the old dull needles when accessing established buttonholes.
The battle between the use of sharp and dull needles became part of the usual difficulties associated with buttonhole cannulation. I have now utilized this proven technique for nearly five years. In that time, I have been able to establish reliable tracks that worked well for weeks or months, but inevitably, I would have to every once in a while use a sharp needle even on the best buttonholes. Over the last six months, my arterial site needed more frequent cannulation with sharps.
I had heard of "Touch Cannnulation" in the last two years, but had done well learning how to place my dull buttonhole needles following the same exact angle each time. Initially, I had no reason to try to refine my technique any further, it had worked well the overwhelming percentage of attempts. The last few months changed my attitude and I reconsidered the Touch Cannulation method when I needed to use sharp needles more and more frequently. I was skeptical it would work but decided to try it out of frustration of frequent sharps cannulations. (Please review the detailed directions by Stuart Mott on how to perform Touch Cannulation in the link above.)
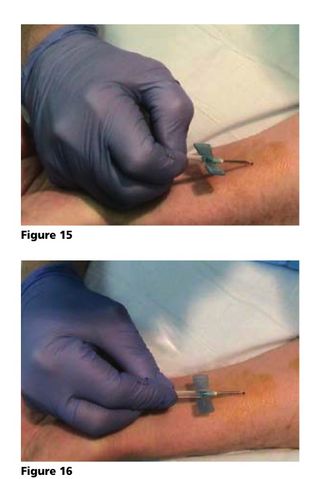
To my greatest surprise, not only did holding the tubing behind the "wings" of the dialysis needle work but it worked well. I have now been using Stuart Motts' Touch Cannulation for over three weeks and the method has worked each and every time. All it takes is to place your thumb and index finger behind the wings on the tubing and line up the right angles and then let the needle find its own path. For those of us who are parents, there may be an object lesson for us to learn as well about guiding but letting them when at the right age seek their own ways in life.
My skepticism has now come full circle to enthusiastic support of this little known method. Stuart Mott continues to be the most sought after expert on cannulation and with good reason. I wish to personally thank Stuart for helping me overcome one of my own difficulties that added to the stress and discomfort of dialysis. My wife also appreciates the ease of cannulation and being able to avoid sharp needles once you have an established buttonhole track.
This may also prove to be one of the solutions to the difficult problems of utilizing buttonhole cannulation in an in-center dialysis unit where multiple techs over time will cannulate the patient. Many units disparage the buttonhole method because it is operator dependent. I suspect that if the Touch Cannulation method were applied widely, the disparity between different cannulators may disappear if everyone involved learns how to let the needle find its own way. With the Touch Cannulation method, that is exactly what the needle does each and every time. The only complaint I have is that I did not try it sooner.
Comments
Emilio E Hughes
Feb 14, 2023 11:39 AM
Peter Laird, MD
Feb 15, 2023 6:28 AM
But yes, I use it even when establishing a new buttonhole as well.
I am not sure what you mean by rotating the site. The Rope-Ladder method is a single puncture and then moving the next puncture site by a couple or few millimeters.
The Buttonhole Cannulation, also called Constant Site Cannulation was the the serendipitous discovery of Twardowski in the 1970's through reuse of needles that eventually became dull.
"History of the Buttonhole Technique
Madhukar Misra
PMID: 26283554 DOI: 10.1159/000431159
Abstract
The constant side method of access cannulation in hemodialysis, popularly known as the 'buttonhole' method, has an interesting history. Dr. Zbylut J. Twardowski, a Polish nephrologist, discovered this technique by pure serendipity in 1972. A patient with a complicated vascular access history and limited options for cannulation was repeatedly 'stuck' at the same sites by a nurse. Soon it was noticed that the cannulation at the same spot became easier with time. Since the needles were being reused, the sharpness of the needles decreased with time and the bluntness of the needle seemed to minimize the damage to the cannulation tract (another serendipity!). This method soon became popular among patients, and many patients started using this technique. This chapter traces the invention of this technique and its subsequent development following Dr. Twardowski's emigration to the USA.
© 2015 S. Karger AG, Basel.
https://pubmed.ncbi.nlm.nih.gov/26283554/
Stuart Mott has had many innovations in cannulation technique among which is the Touch Cannulation technique where you simply hold the flexible tubing below the wings instead of "man handling" the wings on the dialysis needles which gives the patient more control on finding the true buttonhole tract and not creating a false tract.
What I marveled at the first time I used Touch Cannultion and for all the years since, is that it truly improves cannulation success with buttonholes. Hats off to Stuart for all of the innovations and perhaps thousands of patients he has taught to be self reliant and independent.
Peter Laird, MD
Feb 14, 2023 5:59 AM
And it is actually easy to use and become accustomed to the technique rapidly. In my case, I was hooked after the first time I used the technique. I hope it works as well for you as it has for me for quite some time.
Jeffrey R. Stumpe
Feb 14, 2023 5:36 AM
In July 2012 I began hemodialysis as an HHD training patient with my spouse as care partner at DaVita Bluemound At Home. Three of the many objectives of the training were to establish a single set of buttonhole sites, learn "soft touch" cannulation with BH dialysis needles and to cannulate myself with BH dialysis needles. I also learned through observation how to cannulate with sharp dialysis needles, a skill set that became essential in less than 9 months of conducting HHD.
Those skills have served me well over the past 10-1/2 years, through 5-1/2 years of full-time employment with unplanned and planned travel, and through the past 5 years of combined full disability (ESRD - 2012 - Present) and subsequent retirement.
I established my first buttonhole in April 2013 some two weeks before the flap in my AVF on one of the two buttonholes established during my extended training in 2012 had shifted (developing AVF) so that it had become so far out of alignment with the track that no straight needle could reach it. If I had not been proactive in the establishment of a 3rd buttonhole site, I would have had to conduct HHD treatments for the next two weeks with sharp needles and same site cannulation to establish a new buttonhole site.
This lesson was not lost on me. By August 2014 I had established 3 new buttonhole sites, and two replacements for original sites that could no longer be used. I have had to re-establish one of these sites almost annually owed to AVF development (I have a very unique 3 vessel forearm AVF originating from a single anastomosis in my right wrist).
One of the five sites was a reverse needle buttonhole at the dead end of one of the three AVF vessels. After almost 8 years of use it suddenly clotted off, forcing me to abandon the site and that unusable portion of that vessel. One of the remaining sites can only be used for arterial. The remaining 3 sites may be used as either venous or arterial without concern for recirculation owed to locations on two separate venous return vessels.
I am naturally a strong proponent of "soft touch" buttonhole cannulation and the establishment (if possible) and use of more than two buttonholes. I have not missed a single (over 2000) HHD Tx since I "went home" from HHD training in early September 2012. This in spite of flu w/fever, fever from COVID-19 vaccinations & boosters, fractured right thumb and assorted other physical ailments associated with aging.
My 3 vessel 5 ea. and then 4 ea. buttonhole AVF will never be the cause of a missed Tx. Even a clot on one of two venous return vessels will not stop me because I have a second fully functional venous return vessel and up to 3 other buttonhole sites to use until I have a fistullogram and declot performed by my Vascular and Interventional radiologist, whom I've seen nearly annually for the past 10+ years for AVF fistullograms and declots.
Trish McCarron
Feb 13, 2023 7:37 PM
Jeffrey R. Stumpe
Feb 15, 2023 5:23 AM