Blood Pump Speed and Your Dialysis Fistula
Article by John Agar, MD
Barwon Health, Geelong, Australia
www.nocturnaldialysis.org
How do blood pump speeds vary from country to country, and does blood pump speed affect your arteriovenous fistula (AVF)? In the US, blood pump speeds are often in the 400-450ml/min range. In Australia, Japan, and Europe, blood pump speeds tend to be lower, often just 250-300ml/min.
In my view, the higher flow rates that are common in the US are mainly used to allow for shorter dialysis. There are now overwhelming data that shorter treatments are linked with worse overall outcomes. But, can higher blood pump speeds—on their own—harm an AVF?
Sadly, there is a dearth of data on this topic. This is surprising, given how central blood access is to dialysis—and, an indictment of us as dialysis professionals for having largely ignored this vital issue.
Indeed, there is embarrassingly little true research on most aspects of AVF care. So, the answer here is long on theory and short on fact and science.
"Normal" AVF Flow
Transonic™ flow data suggest that total AVF flows above 600 ml/min are enough for dialysis. I prefer to see (and we use) a cutoff of 750 ml/min. In fact, ideally, we aim for a flow of ~1000 ml/min. If an AVF flow falls by 25% or more in any given 4 months, this should trigger AVF exam with ultrasound or a fistulogram. Flows can be too high, too—most see 2000 ml/min as too high.
Table 1 shows two examples of fictional AVF flows—one the "US", one "Europe/Japan/Australia." As you can see, even though they have the same total flow, they differ quite a lot.
| AVF Function | US | Europe, Australia, Japan |
|---|---|---|
| Total AVF flow | 1000 ml/min | 1000 ml/min |
| Arterial needle draw | 450 ml/min (US mean) | 300 ml/min (Aust. mean) |
| Venous return | 450 ml/min | 300 ml/min |
| Segment of AVF between needles | 1000 - 450 = 550 ml/min | 1000 - 300 = 700 ml/min |
AVF flows are more complex than I have made them out to be here. But, the segment of AVF between the needles (See Figure 1) must have less flow since some of your blood is sent through the machine by your arterial needle.
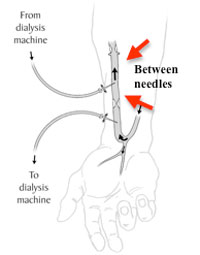
Let's say your total AVF flow is 1000 ml/min. Your (US) arterial needle draws at a higher rate (450 ml/min) than it would in Australia (300 ml/min). This means that the segment between the needles must have a lower flow rate (US: 550 ml/min).
How might this affect your AVF? To my mind, there are two main risks to having higher blood flow rates: blood clots and possible tissue damage to your fistula.
Fistula Clotting
If the flow of blood between your needles is sluggish, it might lead to blood clots. This would seem more likely in the US, at just 550ml/min, than outside the US, where between needle flows are more in the range of 700 ml/min.
But what if your AVF starts out with a flow of just 600ml/min? In the US, "donating" 450 ml/min to the dialysis circuit would leave a flow of just 150ml/min between the needles. (Outside of the US, "donating" 300 ml/min to the circuit would leave a better—though still low—flow of 300ml/min between the needles.)
In the US, a very low flow like this might be enough to clot an AVF. The risk is higher if the hemoglobin level is over 13 g/dL (often aided by EPO), making clots even more likely.
Fistula Wall Damage

Turbulence—unstable flow—always occurs where the venous blood returns. In theory, this turbulance should be greater if the flow (read force) at which the venous needle returns blood is higher. The higher the blood pump speed, the greater the turbulence. This is one reason for vessel wall damage.
Vessel wall damage in your AVF can cause scarring. These scars can lead to stenosis (narrowing). Stenosis, in turn, makes the AVF less able to "drain" towards the heart. Having stenosis raises the risk of a higher venous pressure, recirculation in your access, and poor treatment.
Show Me the Data
Where is the proof? Appallingly, there is little or none! Level A evidence (from randomized, controlled trials) is nil. Even good Level B evidence (from case control or observational studies) is lacking. All that remains is Level C evidence (wholly unscientific and based on opinion—like this article!), and even that is scant.
 Are there any effects of high AVF flow rates in the rest of the body? Again, what follows is opinion only. It is hard to imagine how it could be proven one way or the other. AVF flows
should
be the same "upstream" of the needles as they are "downstream"—at least once the turbulence has settled.
Are there any effects of high AVF flow rates in the rest of the body? Again, what follows is opinion only. It is hard to imagine how it could be proven one way or the other. AVF flows
should
be the same "upstream" of the needles as they are "downstream"—at least once the turbulence has settled.
Some believe that left ventricular hypertrophy (LVH) might result from higher AVF flows. 1 High total fistula flows can increase the workload on the heart. This may promote a state known as "high output failure." 2,3 But, I can see no direct way by which the pump speed of the machine might affect this.
Perhaps other effects may result, though. Here, I go back to my views about the harmful effects of shorter, more "gung-ho" dialysis. The short treatments made possible by raising the pump speed, in my view, yield poorer dialysis and can lead to worse health and lower survival.
References:
- LVH: Heading off a common heart problem; accessed August 2011.
- Basile C, Lomonte C, Vernaglione L, Casucci F, Antonelli M, Losurdo N. The relationship between the flow of arteriovenous fistula and cardiac output in haemodialysis patients. Nephrol Dial Transplant. 2008 Jan;23(1):282-7.
- MacRae JM, Pandeya S, Humen DP, Krivitski N, Lindsay RM. Arteriovenous fistula-associated high-output cardiac failure: a review of mechanisms. Am J Kidney Dis. 2004 May;43(5):e17-22.